Top Stories On FM 7-0: Mobile training teams help units with training management programsBy Training Management Directorate June 23, 2021 
247th Birthday of the United States Army
June is National PTSD Awareness Month
March 19, 2022 Virtual Brain Awareness Day Every workplace can be a place of continual learning
Employers can tap technology to offer higher education to their workers, by
Joe Schaefer
All active-duty Soldiers to pin on corporal after BLC, promotion boards By Joseph Lacdan, Army News Service June 4, 2021 Share on Twitter Share on Facebook Share on Reddit Share on LinkedIn Share via Email WASHINGTON Soldiers soon will shoulder the responsibilities of noncommissioned officers earlier in their careers, following a new Army directive that will promote all junior enlisted members to the rank of corporal prior to making sergeant. Beginning July 1, all Soldiers with the rank of specialist who have been recommended for advancement by a promotion board and completed the Basic Leader Course, or BLC, will be laterally promoted to corporal, a junior NCO. Soldiers who currently hold the corporal rank must qualify for the promotion board and graduate from BLC to remain corporals, or they will be laterally assigned back to the grade of specialist. Further, Soldiers who meet the requirements will wear the corporal rank regardless of the designated grade of their assigned duty positions as they make the transition to the NCO corps. Soldiers will not receive additional pay when making corporal, nor will they lose any of their base salary if they transition back to specialist, said Sgt. Maj. Kenyatta Gaskins, Directorate of Military Personnel Management sergeant major. The directive will apply to active duty Soldiers and Active Guard Reserve members. The instruction will apply to the Army Reserve starting Oct. 1. We want to get after leading, teaching and mentoring our junior enlisted Soldiers early, Gaskins said. This is a junior leader development process and that's how we're looking at this. In the past, the Army selected Soldiers with leadership potential to higher graded positions to become corporals. Now Soldiers who have been recommended for promotion to sergeant and completed the required training will have that distinction. Gaskins said that the length of time a Soldier spends as corporal will vary but each Soldier will be expected to wear the rank for a period of time before transitioning to sergeant. This is a change in culture, Gaskins, who held the rank of corporal earlier in his career. This is not something were used to. The change coincides with the Armys plans to invest more in the leadership development of younger Soldiers, supporting Sgt. Maj. of the Army Michael A. Grinstons This is My Squad initiative. That effort includes a push to further strengthen the Armys junior NCO corps, and will instill more than just leadership skills. Promotion boards to sergeant and staff sergeant include situational-based questions on sexual harassment, misuse of drugs and alcohol and suicide prevention. Soldiers will also be quizzed on suicide prevention, physical fitness, and mental health to gauge their reaction to such incidents and to make sure they can care for Soldiers in those situations. Under the directive, unit cohesion will be strengthened at the lowest levels by promoting Soldiers to corporal. We rely on junior leaders to build cohesive teams that are highly trained, disciplined, and mentally and physically fit," Grinston said. "In many cases, a specialist is charged with that responsibility. This allows us to recognize their role as a noncommissioned officer and ensure theyre getting the coaching and mentorship they need to be successful. Gaskins said by developing leadership traits earlier in military careers, Soldiers will be able to identify and prevent what Army senior leaders have labeled as corrosives to the force including sexual assault and harassment, discrimination and suicide. The Army also announced that beginning June 1, 2022, for active duty, and Active Guard Reserve Soldiers and Oct. 1, 2022, for Army Reserve, Solders must be recommended by a promotion board to Sergeant before attending BLC. Instilling leadership early One of the oldest ranks in the Army, the Corporal rank has been called the backbone of the Armys NCO corps, Gaskins said. Corporals earn E-4 pay but outrank specialists having the distinction of being NCOs. The Army charges them with leading the Armys smallest units, teams of Soldiers, while overseeing the care, training and readiness of fellow troops. Now the rank carries possibly a greater distinction, one that showcases the Armys commitment to developing responsible leaders early and to combat against misconduct. It's a visual reminder that the Soldiers have transitioned from junior ranks to become a member of the NCO Corps, Gaskins said. Related links: U.S. Army ranks Army News Service ARNEWS Archives Combined Arms Center Commanding General visits MEDCoE By Tish Williamson | U.S. Army Medical Center of Excellence Public Affairs | Jan. 21, 2021 JOINT BASE SAN ANTONIO-FORT SAM HOUSTON, Texas The U.S. Army Medical Center of Excellence hosted Lt. Gen. James Rainey, commanding general, U.S. Army Combined Arms Center and Fort Leavenworth, Kansas, at Joint Base San Antonio-Fort Sam Houston Jan. 19-20. In a visit planners described as battlefield circulation, Rainey met with key MEDCoE leaders, received an update brief on Army Medicine in large-scale combat operations and conducted leader professional development, or LPD, sessions with unit command teams and Medical Captains Career Course students. Previously aligned under the U.S. Army Medical Command, MEDCoE realigned from MEDCOM to the U.S. Army Training and Doctrine Command, or TRADOC, with operational control under the CAC that began Oct. 19, 2018, and was completed Oct. 2, 2019. MEDCoE is one of the 10 centers of excellence under CAC and TRADOC to include aviation, fires, cyber and intelligence. Before the first LPD session, Rainey in command since December 2019 recognized several Soldiers and civilians who were nominated by the command for excellence. He then thanked attendees for their service and noted that less than one percent of Americans have volunteered to serve something greater than themselves as they all have through their military service. Rainey explained that, if those who serve are the best America has to offer, then those he is being asked to recognize for excellence must be truly outstanding. That is why I never miss a chance to recognize excellence, Rainey said. You are really in the presence of greatness when you talk about the best of this group of people who are willing to serve their country. The Combined Arms Center is the U.S. Army's lead organization for several modernization initiatives to include managing the Army Leader Development and Army Profession Programs. Leaders should focus on doing well personally and developing others, Rainey said to the MEDCoE company, battalion and brigade command teams. MEDCoEs Borden Institute releases teledermatology E-book By Ernest J. Barner | Borden Institute Public Affairs | Jan. 25, 2021 JOINT BASE SAN ANTONIO-FORT SAM HOUSTON, Texas The Borden Institute, an agency of the U.S. Army Medical Center of Excellence at Joint Base San Antonio-Fort Sam Houston, recently released Teledermatology in Military Medicine as a part of its specialty publication titles. The 12-chapter book, released Dec. 17, 2020, covers all major skin diseases from bacterial, fungal and viral infections to bullous disorders, arthropod-borne diseases, and tumors of the skin. Other selected topics include shipboard consults, cold and hot weather factors, and combat-related burns. The unique factors affecting dermatologic care in each major geographical command are discussed. Representative cases and more than 620 color images are included in this book to demonstrate instructional sample cases from each region. The foreword was written by Lt. Gen. Raymond S. Dingle, U.S. Army Surgeon General and commanding general of the U.S. Army Medical Command. This publication captures a piece of history and is basically a testament to the military dermatologists who provided services before the world had smartphones, social media and reliable internet bandwidth, said retired Army Col. (Dr.) Jon H. Meyerle, senior consultant and editor for the publication. Teledermatology and this publication directly contribute to the care of thousands of service members from every region of the globe. The electronic publication exemplifies the continuing readiness commitment to U.S. Soldiers, Sailors, Airmen, Guardians and Marines and is the ideal resource for military dermatologists and providers who operate at home bases and various remote areas of responsibility. The debut edition of Teledermatology in Military Medicine is currently available in PDF and E-book formats on the Borden Institute website at http://www.medcoe.army.mil/borden. A New Way of Training the Armys Flight Paramedics By Gina Cavallaro | U.S. Army Medical Center of Excellence Public Affairs | Aug 2020
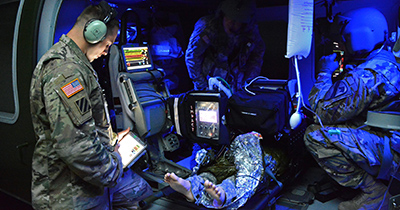
The Army is changing the way it trains its flight paramedics to prepare for a future battlefield where swift medical
evacuation wont be assured. The Combat Paramedic Course, a 30-week pilot, marks the first step in ramping up
medical expertise that could include ground paramedics and more advanced skills for the Armys almost 34,000
combat medics. Jay Harmon III, deputy to the commander of the U.S. Army Medical Center of Excellence in San
Antonio, Maj. Chris Gonzalez, pilot program director, and Master Sgt. Joey Hernandez, pilot NCO in charge, explain.
Their answers have been condensed and edited for space. 2. Do you have an example of that critical thinking? Take something as simple as tourniquet application. We teach combat medics which wounds can be controlled with a tourniquet and then reinforce the accurate, adequate and timely delivery of that. With combat paramedics, we dont just need them to be experts at that kind of basic skill, we need them to understand, OK, I cant evacuate this person for two hours. Can I convert this tourniquet to another kind of dressing thats not going to cut off circulation to the entire limb? Now Ive got them for 12 hours, and I have a new problem. How do I prepare for that? That sort of thing. 3. When will the pilot end? The first course began in January; there were two more starts in March and June, so the pilot will end early in 2021. Our objective is to make it a program of record, build it into the [budget] and make it a recurring and permanent part of our curriculum. Graduates who go on to serve as flight paramedics will attend and eight-week critical care course in San Antonio] and a four-week air crew member training course at Fort Rucker, Alabama. 4. Any additional certifications? Graduates will receive 51 of 60 semester credit hours toward an associate degree in Health Sciences–Emergency Medical Services (Army Paramedic) from the Uniformed Services University, a National Registered Paramedic certificate and [several certifications from national emergency medical and trauma care organizations]. 5. Why just flight paramedics? At this time, the only paramedic requirement is for flight paramedics. If you look at this thing as a pyramid, the critical-care flight paramedics are the very top level. They’re the cap, the most highly trained medic that we are going to put in the force. Army leadership may determine that there are additional requirements for this capability at the ground [level. If so,] we will already have a validated program in place that will simply require resourcing to scale. 6. What’s the next level down on the pyramid? An advanced medical NCO trained to a combat paramedic standard that we would try to employ on all evacuation platforms in certain scenarios, units and situations. We want to make our medics better at the base of the pyramid by giving them more knowledge and more skills that, quite frankly, before have only been seen in our nursing care specialists who receive training in how to take care of patients for longer periods of time. We want to take portions of that [training] to include in Advanced Individual Training for combat medics. 7. How significant is this? It’s the contract that we have with our soldiers that when they go into harm’s way, that we’re going to do everything medically, humanly possible to prevent loss of life. With this, we are just increasing the trust and confidence of the soldiers in us. Army Medical Department Board test auto-injectors, gets feedback from Soldiers By Jose E. Rodriguez | U.S. Army Medical Center of Excellence Public Affairs | Sep 2019 While training during a simulated Chemical, Biological, Radiological, and Nuclear, or CBRN, attack at Joint Base San Antonio-Camp Bullis, a Soldier checks a causality's Mission Oriented Protective Posture, or MOPP, mask. While training during a simulated Chemical, Biological, Radiological, and Nuclear, or CBRN, attack at Joint Base San Antonio-Camp Bullis, a Soldier checks a causality's Mission Oriented Protective Posture, or MOPP, mask. (Photo by Jose E. Rodriguez) Photo Details | Download | 0 RELATED MEDIA Army Medical Department Board test auto-injectors, gets feedback from Soldiers (Related Story) JOINT BASE SAN ANTONIO-FORT SAM HOUSTON, Texas The Chemical and Biological Defense Auto-Injector Device, or CBD auto-injector, is something no Soldier ever wants to use on the battlefield. The effects of chemical and biological weapons are horrific. Nerve agents are the most toxic of the known chemical agents. They are hazards in both liquid and vapor states and can cause death within minutes after exposure. Nerve agents are the primary chemical warfare agent threat because of their high toxicity and effectiveness through multiple routes of entry. They are absorbed through the eyes, respiratory tract, and skin. Ensuring CBD auto-injectors are functional and usable are critical in savings lives. The CBD Auto-Injector Device is designed to be used in a Chemical, Biological, Radiological, and Nuclear, or CBRN, environment. Recently the U.S. Army Medical Department Board, or USAMEDDBD, assigned to the U.S. Army Medical Center of Excellence at Joint Base San Antonio-Fort Sam Houston, conducted a test of these devices at JBSA-Camp Bullis. The Joint Program Executive Office for Chemical and Biological Defense, Medical Countermeasure Systems, or JPEO-CBD MCS, at Fort Detrick, Maryland, requested the AMEDD Board conduct a customer test of the CBD auto-injector device within the operational environment. The data and test findings collected by the AMEDD Board will be will be provided to JPEO--CBD MCS. The CBD Auto-Injector Device is a replacement for the currently fielded auto-injector for treatment against nerve agent and insecticide poisoning, adjunctive treatment, and management of agent-induced seizures. The United States military adopted the auto-injector as the drug delivery device because of ease of use, packaging durability, and drug product stability under varying storage conditions. Soldiers donned Mission Oriented Protective Posture, more commonly known as MOPP protective gear, and tested the CBD auto-injectors in a simulated battlefield exercise complete with smoke grenades. MOPA masks can limit visibility, so the injectors have clear, easy to understand pictorial instructions. "A lot of these auto-injectors used to have wording, just written instructions," said Gary Cabigon, an operational tester with the AMEDD Board. "What we learned over the years is that pictures are easier to comprehend, especially in a stressful environment." Cabigon said that when under a CBRN attack vital seconds saved in dispensing the injector matter. Sgt. First Class Elijah Williamson, an AMEDD Board test officer, talked about conducting the test in the field. "I think it's great having the training asset here at Fort Sam," Williamson said. We have the austere environment where we can create the simulation of the battlefield. We do so much on slides and videos that you want to get hands-on and create that realism out at JBSA-Camp Bullis. You can't get that in the classroom." The CBD auto-injectors are designed to deliver an intramuscular injection with a 22-gauge needle with a pressure-activated coil spring mechanism that triggers the needle after removal of the safety cap. When activated, the needle protrudes through the needle end. The CBD auto-injector device is a replacement for the currently fielded auto-injector for treatment against nerve agent and insecticide poisoning, adjunctive treatment, and management of agent-induced seizures. The United States military adopted the auto-injector as the drug delivery device because of ease of use, packaging durability, and drug product stability under varying storage conditions. To learn more about the Army Medical Department Board's mission, visit https://www.cs.amedd.army.mil/ameddbd.
About MEDCoE
The U.S. Army Medical Center of Excellence, or MEDCoE, is located at Fort Sam Houston, Texas. The Army Medicine proponent responsible to envision and design responsive Army Medicine capabilities and structure that support the fielded force and the future force. We develop adaptive medical doctrine that supports Army and Joint Force operational requirements. As one of the U.S. Army Training and Doctrine Command’s 10 Centers of Excellence, MEDCoE is who the Army relies upon to train, educate and inspire all of its medical personnel. Army Medicine Starts Here! We ensure that Army Medicine is ready today “To Conserve Fighting Strength,” so that Soldiers are able to win our nation’s wars and then come home safely. MEDCoE creates the highest standards of achievement in medical expertise by generating synergy through effective and efficient combination and integration of functions while reinforcing the unique requirements and capabilities of the Army Medical Department. Senior Leadership
Learn More ⟩

CSM Clark Charpentier Command Sergeant Major Learn More ⟩MissionWe envision, design, train, educate and inspire the world`s premier military medical force to enable readiness and strengthen America`s Army. Envision means looking at what the Army`s medical force should look like and what it should be able to accomplish given the missions it can be expected to receive. Design means building the tactical medical units, approving their equipment sets and developing the medical doctrine needed to provide quality healthcare in the field: whether the battlefield or the humanitarian assistance field. Train means providing the education and training to develop military and civilian students into proficient and ready members of the military healthcare team. Educate means through state-of-the-art, hands-on, scenario driven training based on lessons learned from today`s battlefields and clinical settings, we create an environment in which students can develop the educational and training capabilities they will need in order to provide the best casualty and patient care possible. Inspire means the MEDCoE professional staff development and career life-cycle management assures us that students will continue to receive the benefits of the best education and training opportunities available from some of the world`s most capable and innovative instructors, training developers and professional staff members.
VisionTo be the foundation on which Army Medicine is built, sustained and transformed. Our Customers
OrganizationsThere are seven major organizations that comprise the U.S. Army Medical Center of Excellence: The Directorate of Training and Academic Affairs (DoTAA). The MEDCoE is accredited by the Council of Occupational Education, and all programs of instruction are reviewed by the American Council on Education. Students attending courses at the MEDCoE can get undergraduate and graduate college credits. The Graduate School also conducts nine doctoral and five masters degree programs. The 32d Medical Brigade is comprised of the 232nd Medical Battalion and the 264th Medical Battalion. The Medical Professional Training Brigade is comprised of the 187th Medical Battalion and the 188th Medical Battalion. The Directorate of Simulations (DOS) is the central focal point for Army Medical Modeling and Simulation initiatives with the responsibility for the development and execution of medical simulation training and the emerging medical simulated training environment, or STE. The Fielded Force Integration Directorate (FFID) enables the delivery of solutions for the fielded force across the domains of doctrine, organization, training, materiel, leadership, personnel, facilities and policy (DOTmLPF-P) for the Army Health System. The Medical Capability Development and Integration Directorate (CDID) develops future concepts and requirements and conducts experimentation, data collection and analysis to validate those concepts and capabilities. Identifies capability gaps, and develops appropriate requirements to mitigate and close capability gaps for the future. As of 1 OCT 2019, CDID is a subordinate organization of the Futures and Concepts Center (FCC), Army Futures Command, though located at Fort Sam Houston with MEDCoE to ensure synchronization of effort. (LINK: https://armyfuturescommand.com/ The Noncommissioned Officers Academy (NCOA) is our center for NCO professional military leadership education. The Academy teaches courses at both the entry and advanced levels. The Personnel Proponent Directorate (APPD) does force modeling. The Army Medical Department has over 130,000 military and civilian members who work in 200 different officer, warrant officer, enlisted, and civilian specialties. This directorate ensures that the Army`s medical force is properly structured to accomplish the Army Medicine`s many missions. The Army Medical Department Board provides independent operational test and evaluation of medical and medical related materiel and information technology products in support of the Army and Department of Defense acquisition process; provides assessments of emerging concepts, doctrine, and advanced technology applications applied to the delivery of healthcare, both on the battlefield and in fixed facilities.
HistoryThe U.S. Army Medical Center of Excellence (MEDCoE) traces its origin to the Medical Field Service School (MFSS) established, nearly 100 years ago in 1920 at Carlisle Barracks, Pennsylvania. The mission of the MFSS was to train doctors, dentists and nurses in their duties as Army officers. In 1924, the MFSS conducted the first professional courses for noncommissioned officers and privates first class. The MFSS moved to Fort Sam Houston in 1946 and was located in the 9th Infantry Regiment quadrangle; where U.S Army North (5th Army) is now located. In 1972 a reorganization of the MFSS resulted in the re-designation of the MFSS as the Academy of Health Sciences, making it one of the largest medical training institutions in the world. In 1991, it was re-designated as the Army Medical Department Center and School (AMEDDC&S), with the Academy of Health Sciences becoming the school arm of the institution. In 1993, AMEDD Center and School was realigned under the U.S. Army Medical Command (Provisional) and remained under the U.S. Army Medical Command (MEDCOM) as it became fully functional in 1994. On 19 February 2015, to better align with the other education and training institutions across the Army, though still under MEDCOM, the Department of the Army added Health Readiness Center of Excellence to the school’s designation, becoming the U.S. Army Medical Department Center and School, Health Readiness Center of Excellence (AMEDDC&S HRCoE). On 19 October 2018, AMEDDC&S HRCoE began realignment from the U.S. Army Medical Command (USAMEDCOM) to U.S. Army Training and Doctrine Command (TRADOC) with operational control by the U.S. Army Combined Arms Center, to be completed effective 2 October 2019. Effective 15 September 2019, the CoE was finally redesignated as the U.S. Army Medical Center of Excellence (MEDCoE) to further solidify their abiding dedication to Army Medicine, reverence to their profound history, and their commitment towards Army modernization with the singular focus of training Soldiers who will win our nations wars and then come home safely. The MEDCoE supports the Army to lead the design, integration, education, and training of new and innovative approaches to health and the Army Health System. MEDCoE is postured to enable effective and efficient integration and synchronization of Army Medical Department Doctrine, Organization, Training, Material, Leadership, Personnel and Facility, and Policy (DOTMLPF-P) development to ensure the latest solutions to any perceived or predicted Army Medicine gaps are documented and incorporated into our doctrine and instruction. MEDCoE is organized with two brigades to enhance mission command, improve functional alignment, and set the conditions for becoming a degree-granting institution. Each brigade has the responsibility for the execution of training and education, as well as quality of life and immersion into the Army Profession. The CoE structure increases collaboration across TRADOC, other organizations, programs, and the generating force to improve support to the operating force. It embraces best practices and initiatives that improve efficiency and effectiveness of the Army and other Service partners overall. The common structure across all CoEs improves the ability of external agencies to communicate with CoE subordinate elements. Where integrated staffs are realized and common instruction shared, manpower requirements are decreased and greater synergy is gained between staffs and schools. The MEDCoE is focused on the Army and improving the readiness of the force and training the Army’s Medical Professionals. We ensure that Army Medicine is ready today “To Conserve Fighting Strength” by training, educating and inspiring Soldiers and Leaders who are capable of meeting the Army’s requirements for a ready medical force and a medically ready force. Army Medicine Starts Here!
|
|||||
|
|
|||||
| From the Top | |||||
|
Leadership
Notes |
|||||
| Past, Present and Future History of the MEDCoE |
|||||
|
The Call of Duty
|
|||||
| On-line (list of On-line Military Magazines). |
|||||
Army News You Can Use
|
|||||
| Training Notes (training notes, courses, updates). |
|||||
Commentaries
|
|||||
| Medical Medal of Honor Recipients | |||||
|
Photographs/Graphics
|
|||||
|
See What's Happening with Pick a Day (Today in the Department of Defense). |
|||||
|
Editor's Comments
|
|||||
| Disclaimer The concept of the newsletter is to provide training information to military medical personnel and DoD firefighters. |
|||||
| |||||